How to Calculate Peptide Dosage: mg, mcg and Insulin Units
Dr. Sieglinde Klaus
Scientific Editorial Team · Bergdorf Bioscience

Dr. Sieglinde Klaus
Scientific Editorial Team · Bergdorf Bioscience
You calculate peptide dosage in three steps: concentration = peptide amount (mg) divided by added bacteriostatic water (ml), then volume = target dose divided by concentration, finally units = volume times 100 on the U-100 insulin syringe. This guide explains every conversion with concrete numbers and points you to the Peptide Calculator for automatic verification.
In a research context the term describes a pure laboratory arithmetic task: a known powder mass in a lyophilised vial plus a defined solvent volume yields a concentration, from which a desired aliquot is derived as a volume. It is strictly about quantities, not an application recommendation. Lyophilised peptides ship as powder because they are markedly less stable in aqueous solution: hydrolysis, deamidation and oxidation degrade the molecules as soon as water is present (Nugrahadi et al., 2023).
Three quantities form the backbone of every calculation. First the peptide mass, usually 2, 5 or 10 mg, printed on the vial. Second the reconstitution volume, the amount of bacteriostatic water you add. Third the target aliquot, recorded in research documentation as a mass (mg or mcg). From these three values you can fully derive concentration, draw volume and the number of possible draws per vial.
Unit discipline is critical: mass in milligrams, volume in millilitres, concentration in mg/ml. Keeping these axes cleanly separated avoids the most common errors. The entire calculation is deterministic, every number follows necessarily from the others. That is exactly why it maps precisely onto the Peptide Calculator, which uses the same chain of formulas.
Converting between milligrams (mg) and micrograms (mcg, also ug) is the most frequent pitfall, because many research protocols record aliquots in mcg while the vial is labelled in mg. The rule is fixed: 1 mg = 1000 mcg. Accordingly 0.25 mg = 250 mcg, 0.5 mg = 500 mcg and 1 mg = 1000 mcg. To go from mcg to mg, divide by 1000: 500 mcg = 0.5 mg.
A numerical example makes the magnitude clear. A 5 mg vial contains 5000 mcg. If an aliquot of 250 mcg is documented, that equals 0.25 mg, a twentieth of the vial. One vial therefore covers 20 draws of that size on paper. Confusing mg and mcg here misses the target amount by a factor of 1000, a classic decimal error.
The rule of thumb: write all values in the same unit first, before you continue. Convert the vial to mcg (mg times 1000) or the aliquot to mg (mcg divided by 1000). Only then does the concentration calculation follow. This clean separation of units is the foundation for every further step and the point where spreadsheets and the Peptide Calculator safeguard automatically by working consistently in mg/ml.
Concentration is the heart of the whole calculation. The formula reads: concentration (mg/ml) = peptide amount (mg) divided by the added volume of bacteriostatic water (ml). It describes how much active mass sits in one millilitre of the finished solution. Only this number translates the abstract powder amount into a readable volume.
Three examples show the range. Dissolve 5 mg in 1 ml and you get 5 mg/ml, a concentrated solution. The same 5 mg in 2 ml yields 2.5 mg/ml. Dissolving 10 mg in 2 ml gives 5 mg/ml. The peptide amount stays constant; the water volume alone shifts the concentration. More water lowers concentration, less water raises it.
From this follows the draw volume: volume (ml) = target dose (mg) divided by concentration (mg/ml). At 2.5 mg/ml with a 0.25 mg aliquot you get 0.25 / 2.5 = 0.1 ml. At 5 mg/ml the same aliquot would be only 0.05 ml, half the liquid for the same mass. This inverse relationship explains why the choice of water volume directly governs readability on the syringe. Anyone checking the math by hand and then cross-verifying in the Peptide Calculator spots input errors instantly. A detailed step-by-step preparation is covered in the guide reconstituting peptides.
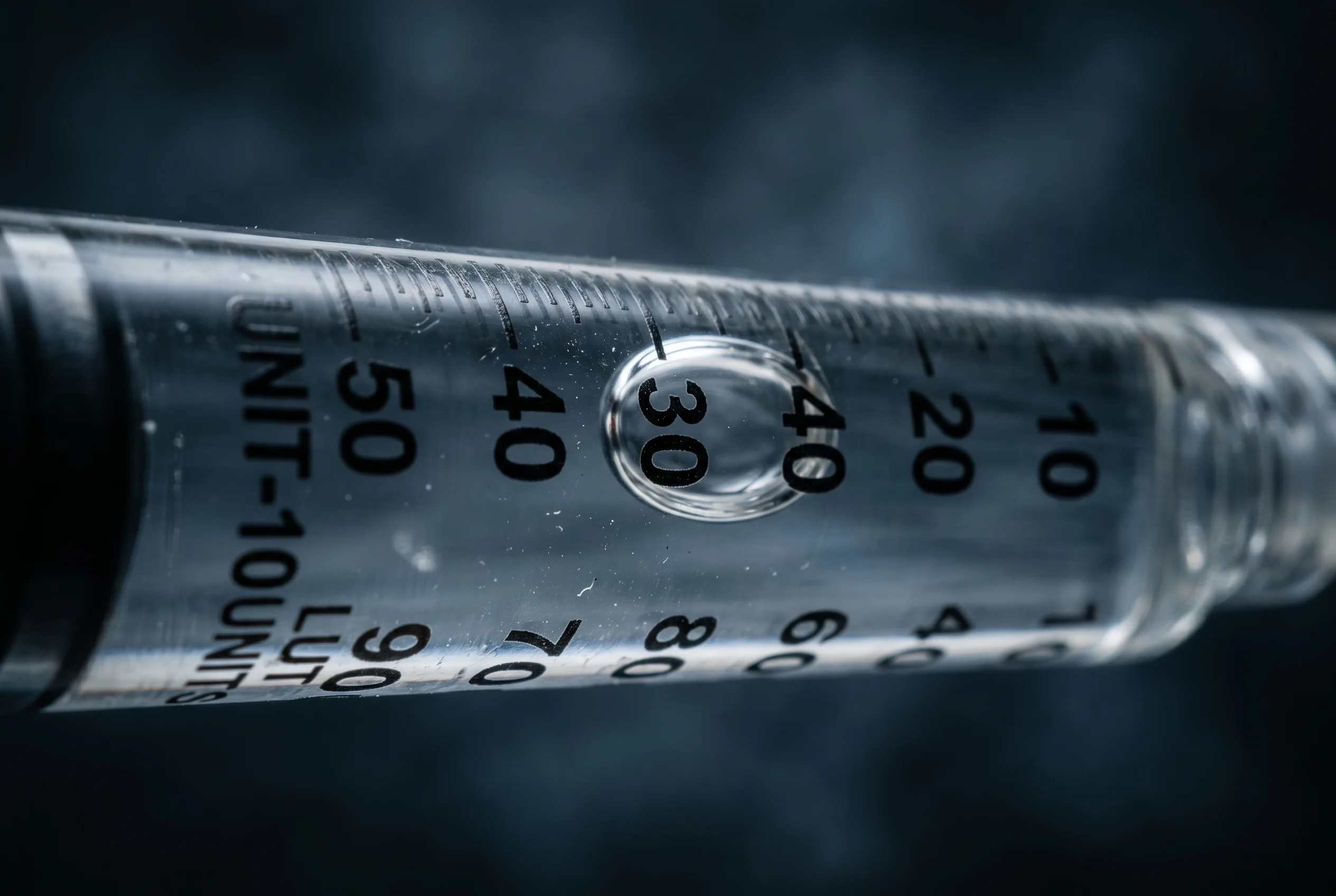
The U-100 insulin syringe is the standard tool for small volumes in the research lab. The designation U-100 means a scale of 100 units per millilitre: 100 units therefore equal exactly 1.0 ml. This standard was introduced historically to reduce confusion between different concentration standards and syringe types (Hartman, 1980). It is precisely this standardisation that makes the conversion between volume and units so reliable.
The scale divides the millilitre into 100 steps. From this it follows directly: 10 units = 0.1 ml, 25 units = 0.25 ml, 50 units = 0.5 ml and 100 units = 1.0 ml. One unit equals 0.01 ml. These lines are marked on the syringe barrel as fine ticks, often labelled every 10 units. It is essential to read a U-100 syringe only with its corresponding scale logic, because other scales interpret the same physical tick differently.
For reading: count the ticks from the zero mark on the plunger side. The plunger edge, not the rubber tip, marks the read position. Hold the syringe at eye level to avoid parallax error. To draw a calculated volume of 0.1 ml, fill to the 10 mark. This direct mapping of volume to tick is the bridge between the concentration calculation and the physical tool.

The final calculation step translates the computed volume into readable units on the syringe. The formula is straightforward: units = volume (ml) times 100. Since 100 units equal 1 ml, you simply multiply the volume computed in millilitres by the factor 100. The result is the tick number you draw up to.
A complete worked example connects all the steps. Setup: a vial with 5 mg of peptide, reconstituted with 2 ml of bacteriostatic water. Step one, concentration: 5 / 2 = 2.5 mg/ml. Step two, the research protocol records an aliquot of 250 mcg, equal to 0.25 mg. Step three, volume: 0.25 / 2.5 = 0.1 ml. Step four, units: 0.1 times 100 = 10 units. You draw up to the 10 mark.
A second example with a different dilution. The same 5 mg vial, this time dissolved in just 1 ml, gives 5 mg/ml. For the same 0.25 mg aliquot it follows that 0.25 / 5 = 0.05 ml, so 5 units. The higher concentration halves the tick count and makes the reading finer, but also more error-prone at small volumes. The Peptide Calculator runs exactly this chain automatically and additionally shows the number of draws per vial, here 5000 mcg divided by 250 mcg = 20 aliquots.
The choice of reconstitution volume is the only freely selectable parameter and determines how well small aliquots can be read. Since the peptide mass is fixed by the vial, the water volume alone controls concentration and thus the draw volume. A larger water volume dilutes the solution, a smaller one concentrates it.
The practical effect shows up at the ticks. Example: 5 mg in 1 ml gives 5 mg/ml; a 0.25 mg aliquot lands at 5 units, very close to the bottom of the scale. The same 5 mg in 2.5 ml gives 2 mg/ml; the same aliquot now lands at 0.125 ml, or 12.5 units, far easier to read. For very small target amounts, more water therefore improves reading precision because the volume is spread across more ticks.
The upper limit is set by the syringe capacity. A U-100 syringe holds a maximum of 1 ml, or 100 units. Computed volumes above 1 ml cannot be drawn in one pull. If the computed volume falls below about 5 units, the solution is too concentrated for that aliquot; above 100 units, too dilute. The Peptide Calculator warns automatically when the volume exceeds the chosen syringe size and suggests a suitable format. This lets you choose the water volume deliberately for a comfortably readable tick count.
For the pure quantity calculation, only the volume of added water matters, not its chemical composition. Whether you add 2 ml of distilled or bacteriostatic water, the concentration formula stays identical: peptide amount divided by volume. The choice of solvent, however, affects the shelf life of the finished solution and therefore over what period the calculated concentration remains valid.
Bacteriostatic water contains 0.9 percent, that is 9 mg/ml, of benzyl alcohol as a bacteriostatic additive. It inhibits the growth of bacteria in the solution and is designated as a multiple-dose container for dissolving or diluting substances (DailyMed, Bacteriostatic Water for Injection USP, 2024). This very property as a multiple-dose diluent makes it the standard for vials from which several aliquots are drawn over days or weeks, such as the bacteriostatic water we supply.
A detail from formulation research: benzyl alcohol can, under certain conditions, promote aggregation of proteins during reconstitution of lyophilised preparations, depending on structural damage during freeze-drying (Roy et al., 2005). This has no bearing on the volume calculation, but it does matter for the stability assessment of the solution. Benzyl-alcohol-free water remains the alternative for single-use preparations, while bacteriostatic water sets the multiple-dose standard.
The calculated concentration is a snapshot at reconstitution. Arithmetically it stays constant as long as volume and mass are unchanged. Physically, however, the effectively available peptide mass can decline over time, because degradation pathways reduce the intact molecule. Peptides in aqueous solution are fundamentally less stable than the lyophilised powder (Nugrahadi et al., 2023).
The main degradation pathways are pH and temperature dependent. Deamidation at asparagine and glutamine residues proceeds especially at neutral to alkaline pH, oxidation affects sulfur-containing residues such as methionine and cysteine as well as aromatic residues, and hydrolysis cleaves peptide bonds under acid catalysis. Solubility itself is strongly pH dependent and minimal at the peptide's isoelectric point (Bak et al., 2014). If substance precipitates or aggregates, the dissolved mass drops and the real concentration deviates from the calculated one.
In practice this means: the volume calculation stays correct over the shelf life, but the underlying assumption of a constantly dissolved mass holds only as long as the solution is stored cold, protected from light and without visible turbidity. A cloudy or flocculated solution signals that the calculated concentration no longer matches the real one. The reconstitution date should therefore always be documented so that the validity of the calculation remains traceable.
Most calculation errors arise not in the formula itself but in the units and the reading. The most common error is the mg/mcg mix-up by a factor of 1000. An aliquot recorded as 250 is 250 mcg, not 250 mg, a difference that renders the whole chain useless. Keep all values consistently in one unit before you divide.
The second classic concerns the syringe scale. If a U-100 syringe is wrongly read against a different scale, the same tick yields a wrong volume. Historically this very confusion between concentration standards and syringe types was the reason for U-100 standardisation (Hartman, 1980). Always check that the scale is labelled in units and that 100 units equal 1 ml. Reading at the rubber tip instead of the plunger edge also distorts the volume systematically.
Further sources: air bubbles in the barrel feign a larger liquid volume; a partially undissolved powder amount lowers the real concentration below the calculated value; rounding errors accumulate across several steps. Regulatory reviews of peptide formulation stress that stability and solubility assumptions must be documented explicitly (Niu & Chiu, 1998). The most reliable safeguard is to check every manual calculation against the Peptide Calculator, which maps the full chain from mg through mg/ml to units consistently.
First determine the concentration, then divide. At 2.5 mg/ml: 250 mcg = 0.25 mg; 0.25 / 2.5 = 0.1 ml, that is 10 units on the U-100 syringe. Without a known concentration the conversion is impossible, because mcg is a mass and ml is a volume.
Exactly 50 units. Since 100 units equal 1 ml, multiply the volume by 100: 0.5 times 100 = 50. The 50 mark therefore sits exactly in the middle of the scale on a 1 ml U-100 syringe.
Not for the concentration formula, where only the volume counts. For shelf life it does: bacteriostatic water with 0.9 percent benzyl alcohol is designated as a multiple-dose diluent and is therefore the practical standard for vials with several draws over days (DailyMed, 2024).
Divide the vial amount by the aliquot in the same unit. A 5 mg vial, that is 5000 mcg, divided by a 250 mcg aliquot yields 20 draws. The Peptide Calculator shows this value automatically alongside concentration and units.
For research purposes only. Not intended for human consumption.
Scientific editor: Dr. Sieglinde Klaus
